
FETAL MRI
Over the past 20 years, ultrafast fetal Magnetic Resonance Imaging (MRI) has progressively increased as a prenatal 3rd level diagnostic technique with a good sensitivity, especially when US examination is inconclusive or when a further investigation is required, in order to confirm or improve the diagnosis and to decide on appropriate pregnancy management. CNS anomalies are the most common clinical indications for in-utero MRI, representing about 80% of the total examinations [Fig 1,2,3,4,5]. The examination is recommended from 19 Gestational Age (GA). Before 19 GA, the currently available technology cannot provide sufficient spatial and contrast resolution to add diagnostic information because the fetus is too small; furthermore, the corpus callosum or vermis are not fully developed before 18 GA. The most frequent indications to perform fetal MRI examination include ventriculomegaly, midline and posterior fossa anomalies, cortical malformations, in utero infections, ischaemic-haemorrhagic lesions and twin to twin syndrome.
In addition to the morphological examination using T2 and T1 sequences, Diffusion Weighted imaging (DWI) showed an increasing role. Actually, several studies have been published on the feasibility of DWI to describe fetal development (brain, lung, kidney and placenta) and regarding its role in the evaluation of pathological conditions to obtain functional data and supplementary information as in the evaluation of ischaemic lesions or in twin to twin syndrome. However, diffusion protocols require careful selection of acquisition parameters and adequate post processing of images to compensate for small fetal movements and extract the correct information through the quantification of molecular diffusion parameters of biological water in tissues [Fig. 6]. To this end, a collaboration is active with the NMR and medical physics laboratory of the CNR ISC located at the Physics Dept. of Sapienza.
Recently, IntraVoxel Incoherent Motion imaging (IVIM) model has been adapted to prenatal MR as an innovative diagnostic imaging tool able to study microstructural qualities of fetal developing tissues (placenta, lungs, kidneys, liver...), in particular analysing perfusion phenomena. IVIM model allows to quantify separately the perfusion compartment, (represented by perfusion fraction f and pseudo-diffusion D*) and the diffusion coefficient D (“real diffusion”). D quantifies the diffusion of water molecules in the extracellular space and it is affected by tissue microstructure, D* quantifies the collective motion of blood water molecules in the capillary network, and f quantifies the perfusion fraction.
Several studies have focused the attention on the use of IVIM-DWI sequence to support prenatal diagnosis of fetal and placental developmental pathologies. In pregnancies affected by IntraUterine Growth Restriction (IUGR), IVIM parameters are able to detect placental microstructural impairment of placental parenchyma compared to normal placental tissue. In particular, the perfusion fraction “f” is significantly lower than normal control values in placental parenchyma of IUGR pregnancies [Fig. 4]. Preliminary data on current literature in normal pregnancy suggests that an increase of microvascular perfusion fraction “f” in fetal kidneys and lungs, with no significant changes in diffusion coefficient D, reflects the physiological hemodynamic changes occurring in these organs during prenatal life [Fig.5].
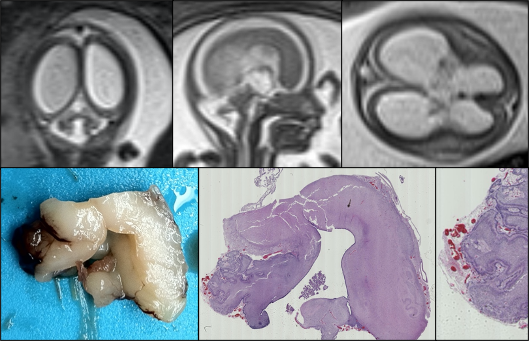
| Figure 1. Fetus at 22 weeks of gestation, Walker-Warburg Syndrome: Magnetic resonance imaging in T2 sequences on the coronal, sagittal and axial planes shows hydrocephalus, ponto-cerebellar hypoplasia with an enlarged tegmento-vermian angle and typical Z-shape appearance of the brainstem. |
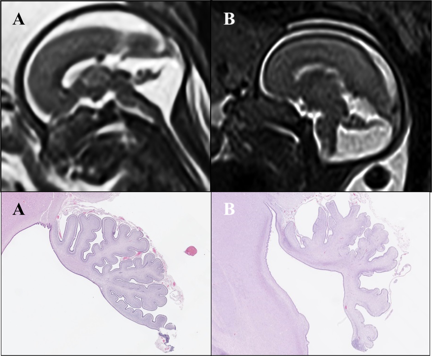
| Figure 2. Dandy-Walker Malformation (DWM): Fetuses at 21 (A) and 23 (B) weeks of gestation with dorsal-rotation of the vermis with dilatation of the IV ventricle, elevation of tentorium and torcula, widening of the ponto-cerebellar angle (>10°), vermian hypoplasia with deficient lobulation. Lineary hypointensity in T2 WI in correspondence of the inferior part of the vermis (“tail sign”; black arrowhead) is a typical finding in DWM |
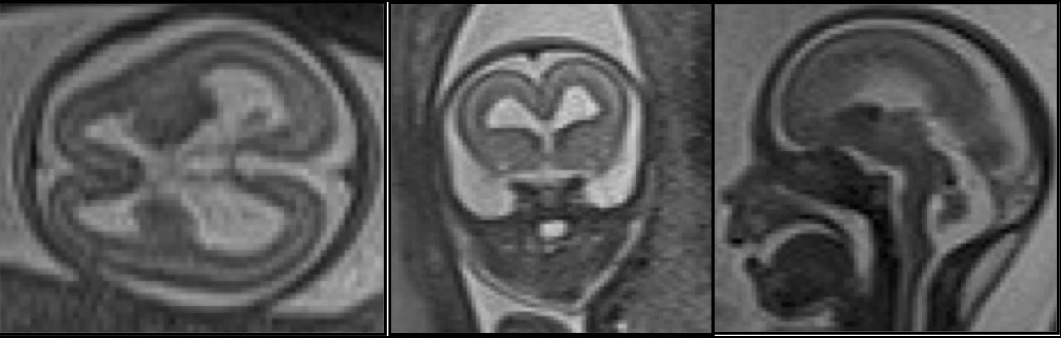
| Figure 3. Fetus at 22 weeks of gestation: Magnetic resonance imaging in T2 sequences shows corpus callosum hypoplasia, ventriculomegaly, cerebellar biometry reduction and cortical anomalies as microlyssencephaly, in relation with a tubulopathy |

| Figure 4. Placental MR with IVIM map (a; b= 0 s/mm2) showing manual ROIs in fetal and maternal side of placenta. b. T2-HASTE on axial plane on placental parenchyma at 35 GA |
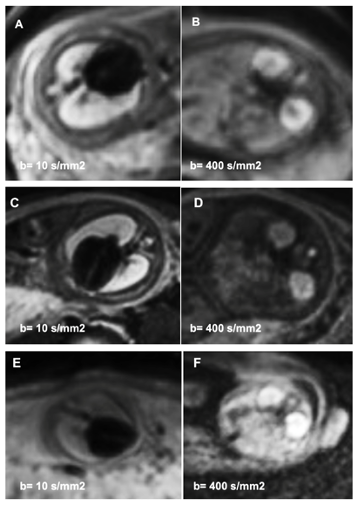
| Figure 5. Diffusion-weighted imaging (DWI) on axial plane of lungs and kidneys in fetuses at 34 GA (A, B), 32 GA (C, D) and 21 GA (E, F). Images are displayed at different b-values: b= 10 s/mm2 for lungs (A, C, E), b= 400 s/mm2 for kidneys (B, D, F) |
| Figure 6. Scheme of image analysis. (A) Raw images were first corrected for noise, Gibbs, and motion artifacts. (B) Seven ROIs were manually drawn. (C) 3 fitting procedures to evaluate perfusion effects of DWI signal: 2 mono-exponential fit (with b-values =50, 200, 700 s/mm2 and b-values = 0, 50, 200, 700 s/mm2) and an IVIM fit (with b-values = 0, 10, 30, 50, 100, 200, 400, 700 s/mm2). The magnification highlights the greater slope of the mono-exponential fit with b = 0 caused by perfusion. (D) Finally, ADC maps were calculated by mono-exponential fit with b-values = 50, 200, 700 s/mm2 (from M.G. Di Trani et al. Front. Phys. 2019) |
References:
- Fetal MRI of the central nervous system: State-of-the-art; L Manganaro, S Bernardo, A Antonelli, V Vinci, M Saldari, C Catalano; Eur J Radiol. 2017 Aug; 93:273-283. doi: 10.1016/j.ejrad.2017.06.004.
- Spatiotemporal expansion of primary progenitor zones in the developing human cerebellum; Parthiv Haldipur, Kimberly A Aldinger, Silvia Bernardo, Mei Deng, Andrew E Timms, Lynne M Overman, Conrad Winter, Steven N Lisgo, Ferechte Razavi, Evelina Silvestri, Lucia Manganaro, Homa Adle-Biassette, Fabien Guimiot, Rosa Russo, Debora Kidron, Patrick R Hof, Dianne Gerrelli, Susan J Lindsay, William B Dobyns, Ian A Glass, Paula Alexandre, Kathleen J Millen; Science. 2019 Oct 25;366(6464):454-460. doi: 10.1126/science.aax7526. Epub 2019 Oct 17.
- Fetal MRI with diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) assessment in the evaluation of renal development: preliminary experience in normal kidneys; L. Manganaro , A. Francioso, S. Savelli, A. Tomei, F. Fierro, M Di Maurizio, F Coratella, A Perrone, L Ballesio, A Giancotti, L Porfiri, M Marini; Radiol Med . 2009 Apr;114(3):403-13. doi: 10.1007/s11547-009-0382-x. Epub 2009 Apr 15.
- Diffusion and perfusion quantified by Magnetic Resonance Imaging are markers of human placenta development in normal pregnancy; S. Capuani, M. Guerreri, A. Antonelli, S. Bernardo, M.G. Porpora, A. Giancotti, C. Catalano, L. Manganaro; Placenta 58 (2017) 33-39. https://doi.org/10.1016/j.placenta.2017.08.003
- Apparent diffusion coefficient assessment of brain development in normal fetuses and ventriculomegaly; M. G. Di Trani, L. Manganaro, A. Antonelli, M. Guerreri, R. De Feo, C. Catalano, S. Capuani; Front. Phys. 7 (2019) 160. doi: 10.3389/fphy
- Diffusion-weighted MR imaging and apparent diffusion coefficient of the normal fetal lung: preliminary experience; L. Manganaro, A. Perrone, S. Sassi, F. Fierro, S. Savelli, M. Di
- Maurizio, A. Tomei, A. Francioso, L. La Barbera, A. Giancotti, L. Ballesio; Prenat. Diagn. 28 (2008) 745–748. https://doi.org/10.1002/pd.2041.
- Fetal brain development at 25-39 weeks gestational age: A preliminary study using intravoxel incoherent motion diffusion-weighted imaging. Yuan X, Yue C, Yu M, Chen P, Du P, Shao CH, Cheng SC, Bian RJ, Wang SY, Wang W, Cui GB.J Magn Reson Imaging. 2019 Sep;50(3):899-909. doi: 10.1002/jmri.26667. Epub 2019 Jan 24
- Microvascular perfusion of the placenta, developing fetal liver, and lungs assessed with intravoxel incoherent motion imaging. Jakab A, Tuura RL, Kottke R, Ochsenbein-Kölble N, Natalucci G, Nguyen TD, Kellenberger C, Scheer I.J Magn Reson Imaging. 2018 Jul;48(1):214-225. doi: 10.1002/jmri.25933. Epub 2017 Dec 27